
BPC-157: Miracle Peptide or Expensive Placebo?
A Croatian Chemist, a Gray Market, and a Placebo Effect Walk Into a Syringe.

I’ve used BPC-157 for one cycle circa 2019 to enhance recovery from an injury.
I recovered from said injury but it’s not really possible to know whether BPC-157 augmented my recovery to a significant degree or if it just happened to be administered while my body recovered naturally on its own.
In other words: it’s possible BPC-157 did nothing significant to enhance recovery such that my recovery pace would’ve been the same without it.
I bought my BPC-157 from Canlab (a Canadian peptide lab); I’m unsure of their quality in 2026 but in 2019 it was good. I didn’t have any significant side effects or lasting reactions and found the process of “reconstitution” (i.e. adding bacteriostatic water to the peptide powder) very easy… bought some injection needles and antibacterial wipes and I was good to go.
If forced to guess… I’d guess that maybe BPC-157 helped a little? And it’s possible it wasn’t even the BPC-157 (could’ve been some hormetic response to an injection or placebo-augmented recovery? or even fluid injected at tendon adhesions to break them up? who knows.)
It’s very easy to placebo yourself with peptides due to the combo of factors that manipulate psychology (animal studies with some evidence, human testimonials claiming it miraculously healed their injuries, injecting something into your body, etc.).
In this piece I’m going to break down the current nuances of BPC-157.
My current thinking is as follows: Most people shouldn’t use BPC-157 in 2026. Unless you have serious injuries with no alternative treatments, the risks and costs outweigh potential upside until stronger/higher-quality evidence emerges to substantiate strong efficacy.

First: What Is a Peptide? Why Does the Word Mean Less Than You Think?
Let’s kill some confusion up front, because “peptide” has become a marketing word that makes people’s eyes glaze over with futuristic optimism, as if the term itself confers some special biological magic.
Many people now think “peptides” are underground natural cures for every biological disease and ailment that “mainstream medicine” doesn’t want you to know about.
A peptide is just a short chain of amino acids. That’s it. Amino acids are the building blocks of proteins. String a few together — roughly 2 to 50 — and you have a peptide. String more together and you have a protein. Your body is full of peptides.
Insulin is a peptide. Oxytocin is a peptide. GLP-1 receptor agonists — semaglutide, tirzepatide, etc. (drugs that are genuinely reshaping obesity medicine) are peptides.
So when someone says “I’m into peptides,” that’s a bit like saying “I’m into molecules.” It tells you almost nothing about what they’re actually taking, why, or whether it works.
The dumbest debate in peptide discourse is arguing via generalization of all peptides: (A) “peptides work” vs. (B) “peptides don’t work.” This is meaningless because each peptide is different.
It’s like saying “pills work” or “liquids don’t work.”
Semaglutide is a peptide.
BPC-157 is a peptide.
One has transformed obesity medicine with massive randomized controlled trials behind it.
The other has three tiny human studies and a cult following on Reddit.
Treating them as members of the same category that rise or fall together is downright stupid. Every peptide must be evaluated on its own evidence, pharmacokinetics, and safety profile.
GLP-1 receptor agonists being revolutionary does not make BPC-157 revolutionary any more than aspirin being safe makes thalidomide safe. They’re different molecules that do different things.
This point matters because the most common rhetorical move in peptide advocacy is to borrow credibility from GLP-1s and transfer it to whatever unproven compound is being discussed.
“Peptides are the future of medicine — look at Ozempic!”
Yes, semaglutide is impressive. No, that does not validate the vial of research-chemical BPC you bought from a website with a “.co” domain.
Something the peptide evangelists don’t emphasize: in traditional pharma, peptides are generally considered the worst of both worlds.
They lack the oral bioavailability and metabolic stability of small molecules (your classic pills).
They lack the target specificity and long duration of large biologics like monoclonal antibodies.
They tend to have short half-lives, poor pharmacokinetics, and a habit of getting chewed up by enzymes before they can do much.
Successful peptide drugs — the GLP-1s, for instance — are heavily engineered.
Native GLP-1 has a half-life of a few minutes and is basically useless as a drug. Semaglutide lasts about a week because Novo Nordisk spent years and billions of dollars modifying it with fatty acid chains and amino acid substitutions to make it survive in the body. (This is one reason many are intrigued by mirror compounds — as mirrors can modify and make unstable short-half-life peptides useful.)
So the fact that some peptides are world-changing drugs does not mean all peptides are interesting. It especially does not mean that a random unmodified peptide you reconstitute from a vial and inject into your deltoid is automatically doing what you think it’s doing.
BPC-157: The Basics
BPC-157 stands for Body Protection Compound-157.
It’s a synthetic 15-amino-acid peptide derived from a protein found in human gastric juice. Or at least that’s the claim.
The compound was first characterized by Predrag Sikirić, a professor of pharmacology at the University of Zagreb School of Medicine in Croatia. He has legitimate academic credentials — 415+ publications, a PhD from Zagreb, an honorary doctorate from the University of Pécs in Hungary. This is a real scientist at a legitimate university.
But there are problems. The vast majority of the published literature on BPC-157 comes from his lab — over 150 papers. And an investigation by Undark, a well-regarded science journalism outlet, found that Sikirić is named on BPC-157 patent applications dating back to at least 1989, is listed as an owner of PharmaCotherapia (the company that sponsored the clinical trials), and is listed as CEO of a company called Diagen which owns a patent for a “special stable version” of BPC-157 that is currently for sale on its website.
These conflicts were not disclosed on any of his published papers that Undark reviewed.
When one lab dominates a compound’s entire evidence base AND has undisclosed financial interests in that compound, that’s a serious red flag. Not proof of fraud — but a setup where bias would be easy and independent replication is conspicuously absent.
And every single one of the hundreds of BPC-157 studies from this lab is positive. A 100% positive publication rate across that many experiments is unusual for any compound.
Does BPC-157’s Mechanism Make Sense?
This is the question worth taking seriously before anything else. Forget the anecdotes for a minute: Does BPC-157 have a plausible story for how it would work in the body?
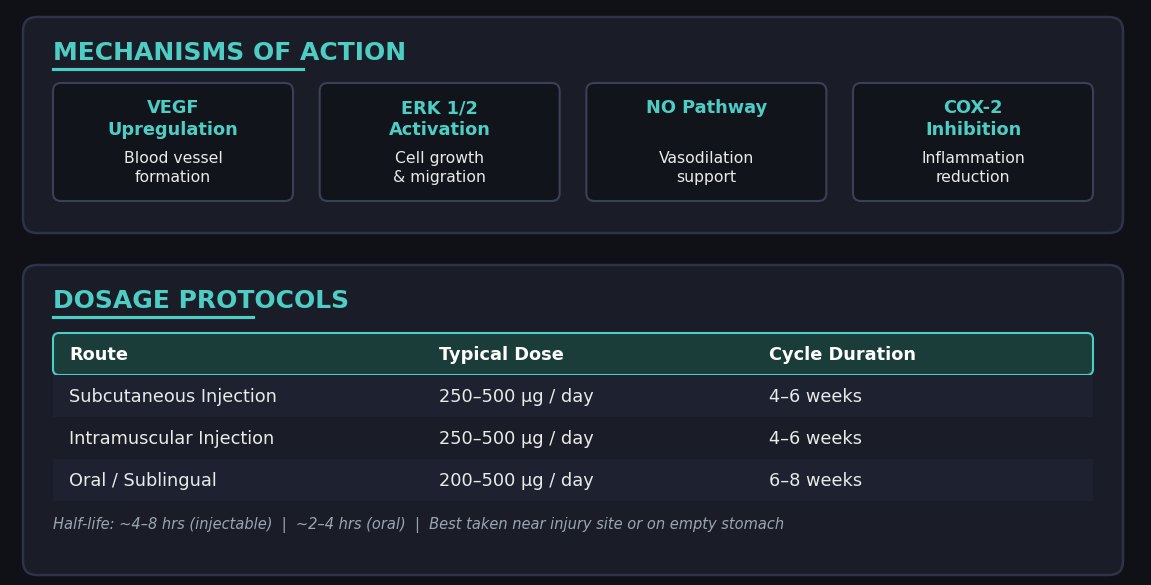
The preclinical (animal) data shows a coherent wound-healing and repair picture: pro-angiogenic signaling through the VEGFR2-Akt-eNOS pathway, tendon fibroblast migration via FAK-paxillin, upregulation of growth hormone receptor expression in tendon tissue, and various anti-inflammatory and cytoprotective effects in gut, muscle, and connective tissue models.
And the animal results against controls are genuinely impressive. The most-cited study (Staresinic et al. 2003) transected rat Achilles tendons and compared BPC-157 to saline over 14 days.
BPC-157 rats showed increased load to failure (how much force before the tendon breaks again), higher Young’s modulus of elasticity (tendon stiffness/strength), significantly better walking function scores, more organized fibroblast and collagen formation under the microscope, and macroscopically smaller defect sizes trending toward full tendon integrity.
Other studies showed similar patterns: muscle crush models had improved load to failure and motor function, ligament transection showed reduced instability and restored biomechanics, and one fracture model performed comparably to bone grafting. In a spinal cord injury study, functional improvements persisted up to 360 days after a single treatment.
Crucially, the core mechanism has been independently confirmed by a team at Chang Gung University in Taiwan — a group with no apparent financial ties to Sikirić. Their in vitro work (Chang et al. 2011, Chang et al. 2014) showed that BPC-157 significantly accelerated tendon fibroblast outgrowth, increased cell survival under oxidative stress, and dose-dependently upregulated growth hormone receptor expression — all confirmed by Western blot and RT-PCR. They declared no conflicts of interest.
This is meaningful: an independent lab at a respected institution validated the cellular mechanism. BPC-157 does something real to tendon fibroblasts in a dish.
Independent replication is partial, not absent — but doesn’t cover the use case people buy BPC-157 for.
Three groups have now worked on BPC-157 independently.
A Taiwan team at Chang Gung University confirmed the cellular mechanism in vitro — specifically that BPC-157 accelerates tendon fibroblast migration, survival, and growth hormone receptor upregulation (Chang et al. 2011, 2014). They studied the right cells (tendon), but in a dish, not in a living animal.
A Chinese team at Air Force Medical University went further — they independently synthesized BPC-157, confirmed its biological activity in vivo in alkali-burn skin wound models and gastric ulcer models, completed preclinical safety evaluations, characterized the full PK profile, and are actively preparing for clinical trials in China for severe trauma and burns. They studied living animals, but for skin wounds and gut injuries — not tendon, ligament, or muscle healing.
Nobody outside Sikirić’s group has put BPC-157 into a living animal, injured its tendon or muscle, and measured whether it healed better versus control. The Taiwan team confirmed the right mechanism in the right cells but not in vivo. The Chinese team confirmed in vivo healing but for skin and gut, not MSK. The specific claims that drive the BPC-157 gray market — accelerated tendon repair, ligament healing, musculoskeletal recovery — remain single-lab findings from a researcher with undisclosed financial conflicts.
Caveats to consider:
Half-life. Animal pharmacokinetic studies show BPC-157 is cleared very rapidly — half-life under 30 minutes, parent drug undetectable after about 4 hours in rats and dogs. A molecule that disappears from your body in hours needs to trigger durable downstream signaling cascades to have a lasting effect. That’s possible — some short-lived signaling molecules do kick off longer repair processes — but it makes the “inject once a day and heal everything” narrative less straightforward than it sounds.
Local vs. systemic. After injection, BPC-157 distributes systemically — but not to where you want it. Animal PK showed the highest concentrations in kidney, liver, and stomach wall (clearance organs), while skeletal muscle levels were comparatively low. So if you inject into your abdomen hoping to heal your shoulder, most of the drug is going to organs that don't need it. This is the argument for injecting directly at the injury site: you deliver a high local concentration to the target tissue rather than relying on weak systemic distribution to get it there.
Effect size. Even if the mechanism is real, we have no idea how large the effect is in humans. A statistically real but clinically trivial acceleration of healing is a very different thing from the dramatic recovery stories on Reddit, X, Substack, and YouTube vlogs. Most biological effects exist on a spectrum, and “mechanistically plausible” tells you nothing about where on that spectrum a compound falls. It could be a 2% improvement in healing time. It could be 20%. We literally do not know.
Translation gap. “Real biology in a rat” and “clinically significant effect in a human” are separated by a canyon littered with the corpses of promising preclinical compounds that failed in humans. The history of drug development is largely a litany of things that worked beautifully in mice and then did nothing — or caused harm — in people.
My thoughts: The mechanism is plausible enough that BPC-157 could have some real biological effect for local tissue repair. But “plausible mechanism” is a low bar.
The Human Evidence: Worse Than You Think
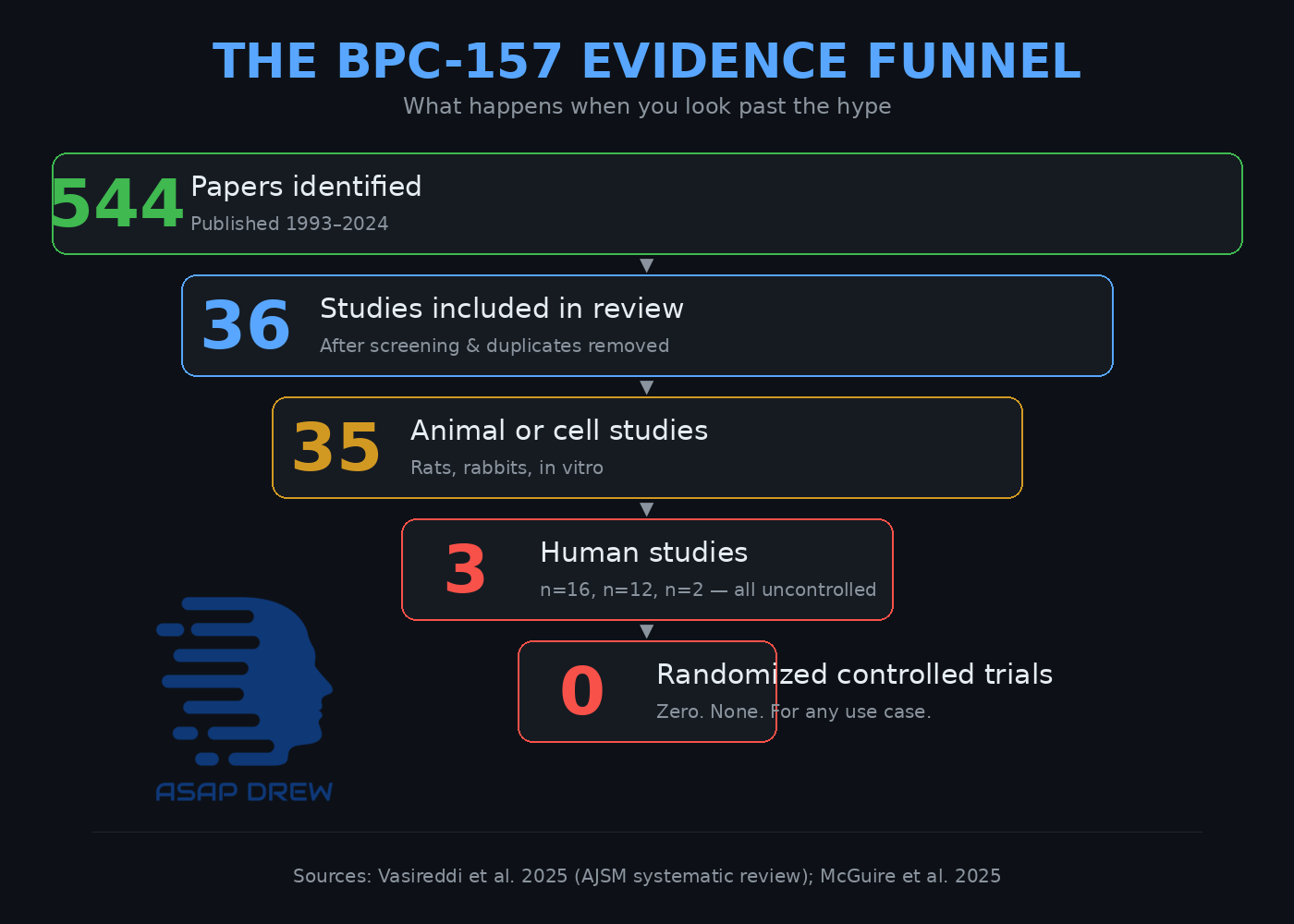
A 2025 systematic review screened 544 papers on BPC-157. Of those, 36 made the final cut. Thirty-five were animal or cell studies. One was a human study. Let that ratio sink in: 544 papers screened, one human study included.
A separate 2025 narrative review identified 3 published human studies total. Here they are:
Study 1: Knee injection. A retrospective case series from a private clinic. Sixteen patients were contacted by phone after receiving intra-articular BPC-157 injections. No control group. No validated functional outcome measures. No blinding. Follow-up was literally a phone call. Seven of twelve surveyed patients reported pain relief lasting over six months. Importantly, this wasn't "I injected and felt better the next day" — patients received a single injection and were then surveyed 6-12 months later by phone, making it a retrospective self-report where placebo, natural healing, and real effect are essentially impossible to disentangle.
Study 2: Interstitial cystitis. A 12-patient pilot study using intravesical (bladder) BPC-157 injections. No control group. Single center. Private clinic.
Study 3: IV safety. A 2-person pilot study looking at whether IV administration was safe. Two people. Not an efficacy trial.
Why we can’t really extrapolate much from these studies:
There are zero randomized controlled trials for the use case people are actually buying BPC-157 for. The entire musculoskeletal healing evidence base — tendons, ligaments, recovery, the stuff that drives 99% of real-world demand — rests on a single uncontrolled phone survey of a dozen patients at a private clinic.
There are zero human studies with imaging endpoints. No MRI or ultrasound. No objective measurement of structural healing in any human study ever published. Every human outcome reported is patient-reported pain — which, as we’ll discuss, is the single most placebo-susceptible endpoint in medicine. Nobody has ever shown, with imaging, that BPC-157 actually changed the structure of a human tendon.
The one actual RCT that did exist was for a completely different indication. A Croatian pharma company called Pliva ran BPC-157 (as PL 14736) through Phase II clinical trials for ulcerative colitis in the early 2000s — not musculoskeletal injuries. The literature references these trials repeatedly as evidence that BPC-157 is “safe in clinical trials,” but the full efficacy results were never clearly published in a peer-reviewed journal. The paper trail consists mostly of other Sikirić papers citing the Pliva trials in passing.
A separate Phase I safety/PK trial was registered on ClinicalTrials.gov — and then canceled. The results were reportedly submitted in 2016, then recalled before quality control review. We don’t know what happened.
To summarize: 544 papers screened. Three tiny human studies, all uncontrolled. Zero RCTs for musculoskeletal use. Zero imaging endpoints. One IBD trial with unpublished results. One canceled registration.
That is the evidence base for a compound people confidently describe as a game-changer.
To be fair: all three published human studies were positive. But all three were also tiny, uncontrolled, and conducted at single sites with obvious investigator enthusiasm. The 2025 review flagged that all published BPC-157 studies are positive, which is a classic publication-bias red flag. In a world where negative results go unpublished (which is the world we live in), a 100% positive publication rate tells you more about the file drawer than about the drug.
Does this mean BPC-157 definitely doesn’t work? No. Does this evidence come anywhere close to establishing that it does? Also no.
We are in the epistemic gray zone where the honest answer is: we don’t know.
BPC-157: Unknown Long-Term Effects and Safety
We have no long-term human safety data. The published human studies are short-duration, tiny, and were not designed to detect adverse effects.
But I want to be logically honest here, because there’s a tension in the skeptical case that most BPC-157 critics don’t acknowledge: if the half-life argument undermines efficacy, it likely also undermines pharmacological risk.
If BPC-157 is cleared so fast (under 30 minutes, undetectable after 4 hours) that it probably can’t do much good, then by the same logic it probably can’t do much harm as a molecule.
We can’t selectively deploy the half-life argument only when it supports skepticism. A compound that’s too short-lived to heal your tendon is probably also too short-lived to cause major harm (e.g. cancer) through direct pharmacological action.
There is a counterargument: short-lived molecules can trigger longer-lasting downstream signaling cascades. A brief VEGF signal could theoretically kick off an angiogenic process that persists for days.
This cuts both ways: if BPC-157 can trigger lasting harmful cascades despite rapid clearance, it could plausibly trigger lasting beneficial ones too.
You don’t get to use “but downstream effects!” only for the risk column.
So what are the real risks? I’d separate them into two categories:
Pharmacological risks (probably low, but unknown). The theoretical concerns about chronic angiogenic stimulation, fibrotic remodeling, and cancer promotion are mechanistically real but also somewhat undercut by the same PK data that makes efficacy doubtful. If you’re using BPC-157 for a short course for a specific injury, the direct pharmacological risk is probably modest. If you’re using it chronically as a daily “optimization” protocol — which some people do — the risk calculus changes because you’re repeatedly stimulating these pathways even if each individual dose is cleared quickly. Chronic repeated exposure is a different animal than a two-week course.
Supply chain and procedural risks (probably the bigger real-world concern). This is where the actual danger likely lives. The FDA explicitly flags immunogenicity risk, peptide-related impurity concerns, and API characterization issues for compounded BPC-157. FDA has documented compounded products made under insanitary conditions. Contamination, wrong product, endotoxins, degraded peptide, potency variation, and self-injection technique failures — these risks have nothing to do with BPC-157’s mechanism and everything to do with the unregulated delivery system. Even if the molecule itself is pharmacologically benign, injecting mystery powder from an unverified supplier into your body is not.
Drug interactions. Zero systematic data on how BPC-157 interacts with other medications, supplements, or other peptides in the multi-compound “stacks” that many users take.
My thoughts: for a short course from a quality-verified source, the direct pharmacological risk is probably low. The supply chain risk is probably higher than the pharmacological risk. And for chronic repeated use, we genuinely don’t know — the absence of reported problems is not evidence of safety, it’s evidence of an inadequate surveillance system.
The Placebo Problem: Why It’s Extremely Easy to Fool Yourself with BPC-157
This is the core of my skepticism, and it’s the same skepticism I apply to myself. When I used BPC-157 and thought “hmm, maybe that helped,” I was stacking every single variable known to amplify placebo responses. Let me walk through all of them, because the number of confounders operating simultaneously in BPC-157 self-experimentation is genuinely extraordinary.
BPC-157’s primary use case in the wild is recovery from musculoskeletal injuries — tendonitis, ligament strains, overuse injuries, joint pain. These are exactly the conditions where placebo effects are largest, most durable, and most convincing to the person experiencing them.
Research has shown that in conditions like patellar tendinopathy, placebo effects from nonsurgical treatments are clinically significant and can persist for up to 12 months. Pain research broadly shows that more invasive procedures generate larger placebo responses, especially for subjective outcomes like “how does your knee feel?”
Here is a non-exhaustive list of every variable working to convince you that BPC-157 is working, whether or not it actually is:
Regression to the mean. People start taking BPC-157 when their injury is at its worst — that’s what motivates them to try something new. But injuries at their worst tend to improve regardless of intervention, because that’s how fluctuating conditions work. You are virtually guaranteed to feel better after starting BPC simply because you started it at a low point. This alone accounts for a huge share of “it worked for me” stories.
Natural healing. Your body heals injuries. That’s what it does. Tendons repair. Inflammation resolves. Tissue remodels. This process takes days to weeks to months and it happens whether or not you inject anything. When you take BPC-157 for three weeks and your tendonitis improves, you have no way of knowing whether the improvement would have been identical without it.
Invasiveness of the procedure. Injection-based treatments generate substantially larger placebo effects than oral treatments. A needle going into your body signals to your brain that something medically significant is happening. The placebo literature on this is robust: the more invasive the delivery method, the stronger the placebo response. BPC-157 is injected. This alone amplifies the perceived effect.
Ritual complexity. This is not popping a pill. You are: researching dosing protocols, ordering specialized supplies (bacteriostatic water, insulin syringes, alcohol swabs), reconstituting lyophilized powder by carefully injecting water into a vial, calculating microgram doses, drawing the correct volume, selecting injection sites, performing the injection with proper sterile technique, and doing this daily for weeks. This is an elaborate, multi-step medical ritual. The complexity and intentionality of the process powerfully reinforces the belief that something real is happening. The harder something is to do, the more your brain insists it must be working — otherwise why would you be doing it?
Esoteric knowledge effect. BPC-157 is not something your average person knows about. You found it through deep-dive research, niche communities, or a cutting-edge doctor. You know things other people don’t. You are part of a group that has access to advanced tools. This “secret knowledge” framing is psychologically potent — it creates identity investment in the treatment working and raises the perceived sophistication and therefore efficacy of the intervention.
Status and authority halo. Peptides are heavily associated with wealthy tech founders, elite athletes, and concierge doctors who charge $1,000+ per consultation. When you see that a successful founder in SF is injecting BPC-157, or that a doctor to professional athletes recommends it, your brain doesn’t process that as “a rich person is also susceptible to placebo.” It processes it as “this person is smart, successful, and has access to information I don’t — they must know something.” This is a massive placebo amplifier. The implicit logic is: ultra-wealthy, high-IQ people with access to the best doctors in the world are doing this, so it must be legitimate. But wealth and intelligence do not protect against placebo effects, confirmation bias, or motivated reasoning — if anything, smart people are better at constructing post-hoc rationalizations for why their expensive intervention is working. The status halo transfers perceived credibility from the person to the product, and it cascades outward: normies see tech bros doing it, tech bros see elite doctors doing it, elite doctors see other elite doctors doing it, and nobody in the chain has controlled evidence.
Financial sunk cost. You paid $50-150+ per vial, plus syringes, bacteriostatic water, alcohol swabs, and possibly a consultation fee. You want this to work. You need it to work to justify the expense. Sunk cost bias is one of the most powerful and universal cognitive distortions, and it operates below conscious awareness. The more you pay for a treatment, the more effective you perceive it to be — this is documented in the placebo literature.
Social investment and identity. You told friends about it. You posted about it. You’re part of the peptide community now. Your identity includes “person who is smart enough to use peptides.” Admitting it might be placebo means admitting you were wrong publicly, and human beings will go to remarkable lengths to avoid that. This creates a community-wide filter where positive reports are amplified and negative reports are suppressed — not by conspiracy, but by ordinary social psychology.
Confirmation bias. Once you believe BPC-157 is working, you notice every improvement and attribute it to the peptide. You ignore or discount the days where pain is the same or worse. You don’t track your baseline systematically. You’re not blinded. You’re not comparing to a control. You are running the least rigorous experiment possible and then trusting your subjective impression of the results.
Concurrent behavioral changes. This is the one almost nobody accounts for. When you start a BPC-157 protocol for an injury, you almost always simultaneously: reduce training volume on the affected area (because you’re “letting the BPC work”), sleep more (because recovery forums told you to), ice or stretch more carefully, pay more attention to form, maybe add other recovery modalities. Any or all of these changes could be responsible for the improvement. You changed five variables and credited the most exciting one.
Subjective endpoints. The primary outcome people use to evaluate BPC-157 is “how does my injury feel?” — a purely subjective self-report. Pain perception is influenced by mood, sleep, stress, expectation, attention, and context. It is the single most placebo-susceptible endpoint in medicine. Nobody is getting serial MRIs to see if their tendon actually looks different. They’re going by feel, and feel is unreliable.
Community reinforcement loops. You go to Reddit or Twitter or a peptide forum. You read 50 posts from people saying it changed their life. You post your own positive experience. Other people read your post and start BPC with even higher expectations, which amplifies their placebo response, and they post about it too. This is a self-reinforcing cycle that produces an overwhelming body of “evidence” that is actually just expectations echoing through a community. Negative experiences get downvoted, dismissed (”your source was bunk”), or simply never posted because people who didn’t notice anything don’t bother writing about it.
Narrative coherence. You’ve read about the mechanism — VEGF, angiogenesis, fibroblast migration and you have a scientific story for why this should work. That story, whether or not it translates to actual human efficacy, makes the treatment feel legitimate and rational. A placebo with a mechanistic narrative feels more real than a placebo without one. Your brain uses the narrative to explain the perceived improvement, creating a self-reinforcing loop of theory and experience.
Every single one of these variables is pushing in the same direction: toward making you believe BPC-157 is working. And they stack multiplicatively, not additively. You are not dealing with one confounder; you are dealing with all thirteen operating simultaneously, in a domain (pain and recovery) where placebo effects are already at their maximum potency.
This is the ivermectin problem. People took ivermectin for COVID, their immune systems fought off the virus over the following days (as immune systems do), and they attributed their recovery to the drug. The same logic applies to chiropractic adjustments, many supplements, homeopathy, and a long list of interventions where the natural course of the condition does most of the work and the intervention takes the credit.
Could BPC-157 still have a real effect on top of all this? Yes. But the point is that the anecdotal signal you see online would look very similar if BPC-157 were a completely inert saline injection. Every single testimonial is fully explainable by the variables above without any pharmacological contribution from the peptide. That doesn’t prove it’s inert — but it means the anecdotal evidence proves nothing either way. I say this as someone who took BPC and felt... maybe better?
The Supply Chain Problem: You Might Not Even Be Getting BPC-157
Even if BPC-157 has real effects, the version you’re injecting might not be BPC-157.
When you order from a gray-market peptide supplier (which is what most people are doing, since BPC-157 is not FDA-approved and not legally available through normal pharmacy channels) — you are trusting an unregulated manufacturer to deliver the correct compound at the correct purity at the correct concentration. The failure modes here are numerous and serious:
You might not be getting BPC-157 at all. Without third-party testing (and most users don’t do third-party testing), you have no way to verify that the vial contains the peptide sequence it claims to contain. It could be a different peptide, a partial sequence, or degraded product.
Contamination. FDA has documented compounded BPC-157 acetate products made under insanitary conditions. Endotoxins, heavy metals, microbial contamination, residual solvents — these are all real risks when manufacturing happens outside of regulated GMP facilities. You are injecting this directly into your body.
Potency variation. Even if the compound is BPC-157, the actual amount per vial can vary wildly from what’s on the label. Under-dosing means you’re getting nothing. Over-dosing means you’re getting more of an uncharacterized compound than you intended.
Reconstitution and self-injection risks. The reconstitution process itself introduces contamination risk if sterile technique is imperfect — which it often is when performed at home. Injection technique matters: wrong needle gauge, wrong depth, wrong site, or insufficient skin prep can cause local infections, abscesses, nerve damage, or injection into the wrong tissue compartment.
This means the real-world risk profile of BPC-157 as actually used is worse than the risk profile of the compound itself. Even if BPC-157’s pharmacology is relatively benign, the delivery system (unregulated manufacturing, unverified product, self-injection) introduces its own layer of risk that has nothing to do with the peptide’s mechanism of action.
Cancer and BPC-157: Everything Unknown
This deserves its own section because it’s the most serious mechanistic concern — and the discourse around it is muddled.
The simple framing you usually hear is “BPC-157 either causes cancer or prevents it.” The more accurate framing is that it could plausibly do both — to different cancers, through different pathways, simultaneously. Biology is not a single toggle.
The pro-cancer concern is the more serious first-principles worry. BPC-157 is pro-angiogenic — it promotes new blood vessel formation. VEGF/VEGFR-driven angiogenesis is a core pathway in tumor growth; tumors need blood supply to expand, and they actively recruit new vasculature. Nitric oxide signaling, which BPC-157 also modulates, plays a dual role in cancer biology and can support angiogenesis, invasion, and metastasis in some settings. So for cancers that are angiogenesis-dependent — which is most solid tumors — you probably do not want to be stimulating the pathways that feed them. If you have an occult tumor somewhere that’s currently starved for blood supply, BPC-157’s mechanism of action is exactly what that tumor wants.
The anti-cancer argument also exists in the literature, but it’s thin. The best skeptical review I found says there are no published in vivo data showing BPC-157 reduces tumor progression, tumor volume, or metastasis. The “anti-tumor” case leans heavily on a single old melanoma cell-line experiment that has never been meaningfully replicated. There are theoretical arguments about nitric oxide’s cytotoxic effects on certain tumor cells, and BPC-157’s anti-inflammatory properties could theoretically attenuate inflammation-driven carcinogenesis in some contexts. But these are mechanistic speculations, not demonstrated outcomes.
The uncomfortable reality is that both could be true simultaneously: BPC-157 could theoretically help protect against certain inflammation-driven cancers while increasing the risk of or bolstering others that are angiogenesis-dependent. Cancer is not one disease. Different tumor types have different dependencies, and a compound that modulates angiogenesis, nitric oxide, and inflammation will interact with each of them differently.
The reality: we don’t know whether BPC-157 is net pro-cancer, anti-cancer, or neutral in humans — and the answer might differ by cancer type. And the half-life consistency applies here too: if BPC-157 is cleared in under 30 minutes, the magnitude of pro-angiogenic signaling from a single dose is probably modest. The concern becomes more real with chronic repeated use, where you’re pulsing VEGF-pathway stimulation daily for weeks or months. For a short course targeting a specific injury, the cancer risk is probably very low. For long-term daily use as an “optimization” protocol, the uncertainty is legitimate.
Either way, cancer history, active malignancy, or unexplained masses should be treated as hard contraindications.
The Incentives: Big $$$ From Selling Peptides
Follow the money, and the BPC-157 hype makes perfect sense regardless of whether the compound works.
For sellers and compounding pharmacies: These compounds are cheap to synthesize, have no patent protection, and can be sold at enormous markups. A vial that costs cents to produce sells for $50-150. Unlike pharma companies, you don’t have to spend a billion dollars on clinical trials first. As AP has reported, clinics are selling consults and shipping peptide kits while these products are still unapproved and often labeled “research use only.” There is also a market positioning incentive: in a world where genuinely innovative new drugs are rare and expensive, “peptides” offer sellers a product category that sounds cutting-edge and scientific while being cheap and unregulated. The term itself does marketing work — it sounds more sophisticated than “supplement” and more natural than “drug.”
For influencers and content creators: Peptides are perfect content. Novel, scientific-sounding, appealing to the optimization-obsessed demographic, and offering a narrative of secret knowledge. Every peptide video, podcast, and newsletter generates engagement precisely because the topic sits at the intersection of aspiration, contrarianism, and scientific-sounding complexity.
For clinics and concierge doctors: Peptide prescribing is lucrative. Patients pay cash. Insurance is not involved. The incentive to believe these compounds work is enormous because your business model depends on it.
For VC-backed startups: This is where the incentives get truly massive. Max Marchione — the peptide advocate from the Shkreli debate — isn’t just a “converted skeptic.” He’s the CEO of Superpower, a health tech company that has raised $51 million in venture funding on the explicit thesis that peptides are the future of consumer health. The company sells peptides and biomarker testing to members, markets itself as building “the AI-Peptide Infrastructure for Mainstream Wellness,” and cites the BPC-157/TB-500 “Wolverine stack” as a core trend it’s riding. Marchione has told interviewers that his employees inject each other with experimental peptides at Friday breakfasts “because we think it’s fun.” When someone with a $51 million company built on peptides tells you peptides work, that is not a disinterested scientific opinion — it is a man whose entire valuation depends on you believing him. This doesn’t make him wrong, but it does mean you should weight his claims accordingly.
For the user community: People who inject peptides have invested time, money, social capital, and physical discomfort into the practice. Admitting it might be placebo is psychologically costly. This creates a community that systematically amplifies positive reports and dismisses skepticism.
The enthusiasm you see online is exactly what you would expect to see whether or not the compound has real efficacy. The incentive structure generates hype independent of the underlying pharmacology.
Why Hasn’t Pharma Picked up BPC-157?
This is arguably the single most damning piece of evidence against BPC-157, and it’s not a study — it’s a revealed preference.
BPC-157 has been known since 1993. That’s over three decades. The pharmaceutical industry is staffed by thousands of people whose entire job is to find molecules that work and turn them into profitable drugs. Drug hunters — people like Shkreli, whatever you think of him personally — scour the global literature for compounds with therapeutic potential. They are ruthlessly incentivized to find things that work, because a compound that genuinely heals tendons or accelerates wound repair would be worth billions.
One company did pick it up — but not for the use case people actually buy BPC-157 for. Pliva, a well-respected Croatian pharmaceutical company, licensed BPC-157 and ran it through Phase II clinical trials for ulcerative colitis (as PL 14736). Not for tendon healing or musculoskeletal recovery… for IBD. Phase I safety data showed it was safe and well-tolerated. A randomized, double-blind, placebo-controlled Phase II study was started. And then... the program stopped. The full results were never published.
What Shkreli and BPC-157 critics leave out: Pliva didn’t just abandon BPC-157 — Pliva ceased to exist as an independent company. In October 2006, Barr Pharmaceuticals acquired Pliva. In December 2008, Teva Pharmaceuticals acquired Barr. The company that was developing BPC-157 was acquired twice in two years and absorbed into Teva, the world’s largest generics manufacturer. Pipeline culling during acquisitions is extremely common — small experimental peptide programs from acquired companies get killed routinely, regardless of whether the compound works. We genuinely do not know if Pliva stopped because BPC-157 failed in Phase II, or because the company got swallowed and the new owners deprioritized a niche peptide program. Both are plausible.
Important: Pliva never tested the musculoskeletal use case — so even if Phase II for IBD failed on efficacy, that would not directly tell us whether BPC-157 heals tendons.
But the broader revealed-preference argument still holds: musculoskeletal healing has been BPC-157’s dominant anecdotal use case for well over a decade.
The preclinical literature on tendon/ligament/muscle repair has been published and available. Drug hunters have had every opportunity to pick this up for MSK indications. Nobody has — though as noted above, an independent Chinese team is preparing for clinical trials for severe trauma and burns, so someone outside Croatia is taking it seriously enough to move toward the clinic. The patent excuse is weaker than people think: you don’t need a composition-of-matter patent to make money in pharma. There’s 5-year NCE exclusivity, 3-year exclusivity for new clinical investigations, 7-year orphan drug exclusivity, and various other regulatory protections. If BPC-157 demonstrably healed tendons in a controlled trial, someone would find a way to monetize it.
The fact that nobody has — after 30+ years of the compound being known, after a pharma company tried it for a different indication then got acquired, after thousands of drug hunters have had the opportunity — is not proof that it doesn’t work. But it is a meaningful signal from the people with the most expertise and the most incentive to know.
What Would Settle the BPC-157 Debate?
If we’re serious about knowing whether BPC-157 works, here’s what a proper study would look like — and the fact that nobody has done it yet is itself informative:
Design: Double-blind, placebo-controlled, randomized trial. This is non-negotiable. Given the strength of placebo effects in musculoskeletal medicine, any unblinded or uncontrolled study is essentially worthless.
Population: Patients with a specific, well-defined injury type where you can get a reasonably homogeneous cohort. Something like partial-thickness rotator cuff tears, or Achilles tendinopathy, or lateral epicondylitis (tennis elbow) — injuries that are common enough to recruit for, specific enough to standardize, and slow enough to heal that you could detect an acceleration.
Objective endpoints: This is critical. You cannot rely on patient-reported pain scores as your primary outcome, because that’s exactly where placebo effects dominate. You need imaging: serial MRI or ultrasound showing structural healing — tendon thickness, tear size, tissue organization, neovascularization. Ideally paired with functional biomechanical testing: grip strength, range of motion, load tolerance. The primary endpoint should be something a scanner can see, not something a patient reports.
Control for confounders: Both groups need identical rehabilitation protocols, identical activity restrictions, identical follow-up schedules. The injection procedure itself should be identical (same volume, same site, same technique) with the control group receiving a saline injection.
Duration and follow-up: Long enough to capture both the acute recovery window (weeks) and any lasting structural difference (months). At minimum 12 weeks, ideally 6-12 months.
Sample size: Powered adequately to detect a clinically meaningful difference — which requires first defining what “clinically meaningful” even means for BPC-157, something nobody has done. A 5% improvement in healing time might be statistically real but clinically irrelevant. You’d want to power for at least a 20-30% improvement in the primary imaging endpoint to justify the cost and risk of treatment.
Independent investigators: Not Sikirić’s lab. Not a clinic that sells peptides. An academic center or CRO with no financial interest in the outcome.
This study would cost a few million dollars. Not billions. If the peptide community is serious — if the companies selling BPC-157 vials and the influencers promoting it really believe in what they’re selling — this is entirely within reach.
The fact that it hasn’t been done tells you something about either the confidence level of the people profiting from the status quo, or the difficulty of the regulatory pathway, or both.
The Debate: Shkreli vs. Marchione
I recently watched a debate between Martin Shkreli and Max Marchione on the broader peptide question, with BPC-157 as the central case study.
Shkreli’s core argument: BPC-157 has no credible human evidence, the preclinical work is dominated by one lab, the compound has terrible pharmacokinetic properties, and the anecdotal evidence is indistinguishable from placebo. His strongest argument was the broader revealed-preference point: BPC-157 has been known for 30+ years, and nobody has taken it through clinical trials for the musculoskeletal use case that drives real-world demand. That's worth noting — though as discussed above, the one pharma company that did try it tested a completely different indication (IBD), then got acquired twice and ceased to exist, so their abandonment doesn't tell us what Shkreli implies it does.
Marchione’s core argument: Thousands of doctors have given BPC-157 to patients for 10-20 years. Millions of patients report life-changing results. His own father went from daily painkillers to pain-free in three days. His cofounder went off biologics for autoimmune disease. The gray market is dangerous, so these compounds should be legalized and regulated rather than driven underground.
Who won on the merits? Shkreli, and it’s not particularly close on the evidence question. His core logical framework — if you claim efficacy, show controlled evidence; anecdotes are not proof; the burden of proof is on the claimant — is simply the correct epistemic standard. Marchione’s case relied heavily on appeal to authority (some trusted doctors use and recommend it), appeal to popularity (thousands of doctors, millions of patients), and appeal to emotion (his father’s pain, his cofounder’s illness). These are powerful rhetorical tools but they are not evidence.
Marchione’s strongest point was the policy argument: a gray market exists, people are already using these compounds, and regulated access through GMP-certified facilities would be safer than the current underground supply chain. That’s a reasonable harm-reduction argument regardless of whether BPC-157 actually works. Shkreli’s response — “I prefer no market” and “we can arrest the genie” — was his weakest moment, but it’s worth unpacking why it was weak, because Shkreli was actually making a strong argument for a different compound and then misapplying it.
Earlier in the debate, Shkreli made a good IP argument about retatrutide — a GLP-1 drug that Eli Lilly is actively spending billions to develop and bring through FDA approval. People pirating that compound through Chinese manufacturers while Lilly is mid-development is straightforward intellectual property theft, and it does undermine the R&D incentive structure that produces new drugs.
You want pharma companies to keep investing in drug development? Then you should respect the IP of drugs they’re actively developing. That argument is smart and something I agree with because it sustains prosperity in pharma.
But for BPC-157, the IP argument evaporates entirely. Nobody holds a patent on it. Pliva licensed it, tried to develop it, and walked away. Sikirić’s lab is an academic research group, not a pharmaceutical company with an investment to recoup. It’s a 30-year-old compound the industry abandoned. There is no intellectual property to protect.
Shkreli gets a bit paternalistic when he says “I prefer no market” for peptides like BPC-157 because the argument is not about IP; it’s: “you shouldn’t be allowed to self-experiment with non-FDA-approved substances.”
That’s a defensible philosophical position but I disagree with it if the substance is relatively safe with potential upside; you should have freedom to do whatever you want with your body. And this is a different argument than he made about reta.
If a compound is unpatented, not being actively developed by anyone, and not FDA-approved, then preventing informed adults from accessing it is anti-freedom.
Regulatory Status: No, Peptides Haven’t Been “Legalized”
As of early 2026, BPC-157 has not been formally legalized for routine compounding in the United States. The FDA currently lists it as a 503A Category 2 substance — meaning the agency has identified significant safety concerns.
FDA warning letters state that BPC-157 is not a component of any FDA-approved human drug and does not appear on the 503A bulks list.
There is political pressure to change this. RFK Jr. has publicly discussed loosening restrictions on certain peptides. But political pressure and completed regulatory action are different things. Policy noise exists; finalized legalization does not — yet.
If You’re Going to Use BPC-157 Anyway
This is not medical advice. But if you’ve read all of the above and still want to try BPC-157, here’s my practical take:
Minimal dose, minimal duration. Do not make this a routine. If you’re going to experiment, use the lowest dose that the community considers potentially effective, for the shortest duration plausible, for a specific injury — not as an ongoing “optimization” protocol. The unknown long-term risk profile means that chronic use is a worse bet than a short targeted course.
Quality-verified sourcing only. If you can’t verify what’s in the vial, you’re not just taking a gamble on efficacy — you’re taking a gamble on contamination, potency, and identity. Third-party certificate of analysis (COA) from an independent lab testing for peptide identity, purity, endotoxins, and sterility is the minimum bar. If your supplier can’t or won’t provide that, find a different supplier or don’t use it.
Local injection makes most sense. The two human efficacy-style studies both used local compartment delivery (intra-articular, intravesical). If BPC-157 has a real tissue effect, the most coherent expectation is local repair signaling in the tissue directly exposed, not distant healing from a random subcutaneous injection.
Accept that you won’t know if it worked. Your experience will be confounded by everything else you’re doing. You will feel like it helped. That feeling is not reliable evidence. Be honest with yourself about this.
The Bottom Line
I don’t know if BPC-157 works. Nobody does. The mechanism is plausible but human evidence is nearly nonexistent. The effect size is unknown (assuming a real effect) and the long-term safety profile is unknown.
The peptide supply chain is largely unregulated. And the entire ecosystem around it is structured to generate enthusiasm whether or not the compound does anything.
The honest label for BPC-157 in 2026 is: unproven peptide with a plausible repair mechanism, almost no human evidence, unknown effect size, unknown long-term safety, and marketing that has wildly outrun the science.
And remember: not all “peptides” should be lumped together. Semaglutide being a success does not make BPC-157 effective. Thymosin alpha-1 being approved in 35 countries does not mean the next peptide on your Instagram, X, YouTube, TikTok, Reddit, etc. feeds are safe and effective.
Just because a random MD (medical doctor) recommends BPC-157 does not mean that it works; without randomized controlled trials we don’t know the actual effect from a placebo response and/or organic recovery.
I’ll update my views (like any logical person should do) on BPC-157 if someone publishes a well-designed, adequately powered, randomized controlled trial in humans; we need this data to know if it actually does anything significant.
Lastly, if and when BPC-157 turns out to be effective and/or safe in the future, some will say: “See! I told you… I knew all along it was effective!” These people are lying and are mostly stupid… they didn’t have evidence, they just guessed correctly.